PART IV: Cognition and Personal Development
9
Impacts of Fear of Authoritative Figures and its Effects
Jasmin Shellenbarger; Sarey Salazar; and Emily Ung
Fear of Authoritative Figures
The topic we are studying concerning cognition is the relationship between fear and schemas. Specifically, the focus of this project is to explore how fear of doctors and those in law is created and its effect on our mind through schemas, which are certain experiences causing the formation of mental maps. The creation of fear is initiated by an external stimulus that triggers a person’s flight or fight response. This causes panic that affects the brain and the connections it makes through neurons, memory, perception, etc. This is an important topic to look into since the fear of authoritative figures, in general, is common in the United States, and can negatively affect various groups of people. One fearful experience can create a negatively impactful schema, which can lead to problems in an individual’s personal life and health.
For instance, an individual who had a negative experience in a medical setting would expect all other situations in that same setting to be scary. This effect creates a negative schema. Patients can then refuse care and omit important information from a doctor, as shown in Figure 1. The fear of doctors is called latrophobia, or white coat syndrome, and it affects approximately 20% of the U.S population as of 2018 (“Chills and Thrills,” 2018). The final goal of our project is to give people a better understanding of the flow of fear and its effect on schema processing. Ultimately, we want to teach others how we can keep a cool head under pressure by changing schemas for the better.
Figure 1. An example of an authoritative figure, such as a doctor.
The Role of Cognition
Cognition is known as the mental processes of how the mind operates, functions, and how it interprets its surroundings through thoughts, behaviors, and senses (Goldstein, 2019, p. 6). Cognition has been examined scientifically through studies of mental processes. In this case, the relationship between memory and perception in the creation of schemas. Researchers use machines such as functional magnetic resonance imaging (fMRI) to see how the brain responds to certain stimuli, which in turn gives us an idea as to how the brain functions under these circumstances. The brain responding to external stimuli is an example of bottom-up processing. An important place to begin is the neural circuits that form in response to an external stimulus (Goldstein, 2019, p. 29). In this instance, during a stressful time, the initial fear of an authoritative figure could be caused by a person abusing their power, causing the first fear pathway in the brain, and creating a schema of authority equating to fear. As a result, the fear of authority begins, and more interactions between an abusive person with prestige can further enhance the schema, ensuring that the neural network will always associate fear and authority. When the schema is activated, it is top-down processing or “Processing that originates in the brain” (Goldstein, 2019, p. 67).
The brain also functions to form schemas through the fusiform face area (FFA; Goldstein, 2019, p. 42), as shown in Figure 2. The FFA is part of the brain that recognizes facial features. Difficult interactions occur with someone higher up can leave a lasting impact on how their facial features and expressions are interpreted through the schema. Memories of when a person was taken advantage of can be brought up when a doctor has a similar face of the feared authoritative figure. Therefore, the FFA is a facial schema maker, and groups people based on facial features. With a negative schema of a bad interaction, it creates an overall fear of anyone physically similar to the original authoritative figure.
Following that, perception occurs in conjunction with action (Goldstein, 2019, p. 61). It involves the coordination of visual representation, determining location, and reaction. Perception is experiences resulting from the stimulation of the senses (p. 60). Bottom-up processing is when an image of the environment is first introduced and transmitted through the eye, and then that information is received in the brain. Vice versa, top-down processing occurs when spreading activation of previous neural networks, activation spreads, and then we come to a recognition of the environment. A term associated with perception is imagery. Images are used for encoding, making imagery detrimental to memory (Goldstein, 2019, p. 312). Mental maps can be created using the memories from those images. The Greek poet Simonides coined the method of “loci,” which means memories are organized “at different locations in a mental image of a spatial layout” (Goldstein, 2019, p. 313). Tying this back to the fear of authority figures, the person would remember their environment, building more negative schema with certain images or specific equipment. For example, if the fear-inducing doctor had a painting of Cocker Spaniel dogs, then just seeing any depiction of the breed outside the original environment would trigger fear.
The brain is still being studied today due to its complexity and many different parts. Meaning, some parts of the mind work together to make sense of different external stimuli. The brain is multidimensional; “even simple experiences involve combinations of different qualities” (Goldstein, 2019, p. 43). This is associated with fear of authoritative figures, specifically doctors, because it implies that multiple stimuli are involved in the creation of negative schemas stemming from fear through neural networks. This can be through both top-down and bottom-up processing. For example, someone could have had a bad doctor that has a distinctive face with a deep voice; thus, that person creates a schema of associating deep voices and similar facial features to the fear they felt with that same doctor.
Emotions are often connected to memories. The temporal lobe is used to remember the audio of the deep voice and facial features as the FFA is activated. The use of multiple parts of the brain is important because it aids in the construction of the big picture. Someone simply hearing a deep voice alone would not do much to stimulate the fear felt with the original doctor who has a distinctive face. However, recognizing the face with FFA coupled with the audio together creates the big picture, a schema, of fear surrounding ‘doctors.’ The multiple uses of different parts of the brain act as context for each other.
Shifting the Schema
There are ways to help shift the schema and fear into a beneficial way of coping. The distinctly impactful memory of a negative situation with a person of power is what originates the schema, and it can take a lot of work to reshape that from long term memory. Long term memory consists of sensing and interpreting new information. The process of sensory stimuli and the interpretation of said stimuli/ information can be summed up as the Working Memory Model. The Working Memory model consists of both semantic and episodic memory. Since memories can be altered each time they are recalled, continually bringing the circumstance into short term memory could potentially modify the memory into feeling worse than it originally was. This would be considered an autobiographical memory, composed of the Self Memory System, as it’s both semantic and episodic (Goldstein, 2019, p. 174). Moreover, it is a combined story of a person. An example might be, someone went to where a person of power works, such as a doctor’s office, this being semantic, and they had a very negative experience, episodic memory.
Emotions also affect how one remembers events as they are often “associated with “special” events (Goldstein, 2019, p. 231). This is because autobiographical memories (a combination of episodic and semantic memories that are often remembered more accurately) are multidimensional and therefore remembered better than other memories (Goldstein, 2019, p. 227). In this instance, the fear of an authority figure causes the original fear-inducing memory to have such a big impact, or memory consolidation, in the creation of a schema. Memory consolidation is the “process that strengthens memory for an experience” (Goldstein, 2019, p. 231). Fear affects what neurons fire and what neurons decide not to fire, thus aiding in memory consolidation. A way to transition away from connecting a location to memory would be to work on altering the neural network connected to that recall.
When a person hears of a negative interaction a friend or relative had, it can influence their image of doctors. Then when that same person is in a doctor’s office or hospital, their attention is shifted back to the memories of what was mentioned to them before, therefore affecting their judgment of the situation. This can lead them to find meaning in places there was none, and read interactions as cold when they were not. It may additionally form a prejudice against health professionals in general.
What is a Wise Intervention?
Wise intervention is an individual and social problem that involves relationships of self with others. It is how people make sense of themselves, of other people, or of a situation that they are in. Some examples include personal and intergroup conflicts, poor health and achievement, low self-esteem, and unhappiness. Wise interventions use theory- and research-based techniques to help people through key concepts that can be altered in brief, distinct ways. In other words, it allows the individual to accomplish their goals, and ultimately have a lasting impact on the person at a personal and social level.
Wise Intervention “Dos” and “Don’ts”
A wise intervention must be based on a psychological theory/process to work. Most studies consist of three major parts: the intervention/theory, intervention/control group, and the psychological process that explains the theory for the experiment (Walton, 2014, p. 74). It is important to note that wise interventions do not work instantaneously. They are “A process that unfolds over time” (Walton, 2014, p. 76). Wise interventions often are used to treat a person with mental behaviors that can be difficult to see instant changes. Also, the context of the targeted population is key when it comes to wise interventions. They have to make sense to the targeted population in three ways; setting, psychological process, and long term effects that “alter critical recursive processes” (Walton, 2014, p. 79). Psychological processes can be altered to help each specific population.
As stated before, wise interventions test theories that do not produce instant results. Changes are seen when studies are over, but it takes time to see the overall long-term effects. Furthermore, context changes based on population as they change “rapidly…in ways that can affect meaning” (Walton & Wilson, 2018, p. 637).
Wise Intervention Article
People tend to have expectations that will alter how they interpret the world to show them exactly what they wanted. Someone who expects a doctor to be mean or scary will only see the doctor in that sense, and any situation they are put in with a doctor will result in them feeling like they were right the whole time. As described in the article Wise Interventions: Psychological Remedies for Social and Personal Problems, the writers explain how children in schools were performing when growth-mindset beliefs were given to them in an attempt to change their success rate in school (pp. 326-237). When the students expected to do well because they believed in themselves, it began shifting their grades. This method can still be used even if the expectancy they had has been disproven. That means, even if the truth comes out that the person believed something false, they will continue to believe it anyway. So, students who do bad on an exam but still believe in themselves will not take it as they are a failure, but will instead see it as a fluke. To adjust a person’s fear of doctors, they must remodel their mental views to change their expectations about seeing a medical professional, which can potentially be shifted with a change in how they see themselves.
There are many ways to influence a person to change how they see a situation. One way would be to make mental symptoms seem like physical responses. This can cause them to feel as though the negative aspects are just natural responses to the situation, meaning they are not bad. An example of this is to have them imagine that feeling overwhelmed or stressed while waiting in a doctor’s office is solely the body preparing itself to go get a check-up to prove the person is healthy. Another way would be to take the self out of those fears. Rather than saying I am afraid of the doctors, which is labeling the self and preventing change, say I have a fear of doctors. This makes it so that the fear is not an attachment to how someone views themselves. Instead, it is a thing that can be changed over time. A different way to help a person with this fear is to have them write about the experiences they had. In the Wise Intervention article, the researchers did a study on college students who had gone through traumatic experiences. The research showed that writing them down benefited them by improving their overall health, by writing about the events as a self-distant perspective, implying it happened to the person, but a distant self-image (p. 627). This means the one writing is not reliving the experiences, but seeing them as if they are a third person. By removing themselves from that negative experience, it can make a person feel separate from their past, as though it no longer defines who they are in the present.
Following on journaling, someone with anxiety surrounding medical help can keep notes on how health-conscious they are, and how important it is for them to feel like their health is in their control. Not only that, but also how relevant health is in their life, and how much better their life is by being healthy. By doing this, along with journaling about past experiences, A person can reframe their autobiographical memories into seeing how beneficial medical professionals are and how necessary they are to keep everyone healthy. By reframing their outlook on doctors, it may make a person less fearful because they understand that seeing a doctor is just something that has to be done.
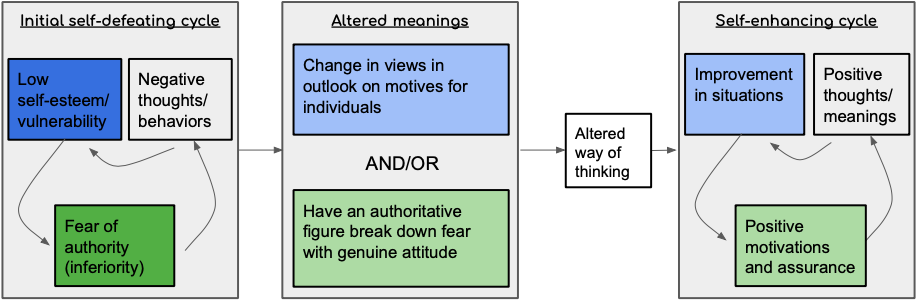
Figure 3. An approach to reform. The situation consists of opportunities for a change in meaning to become embedded in the structure of people’s lives to promote growth and success with relationships.
How is this Solved?
Utilizing the wise intervention logic model, this means that when it’s time to visit a doctor, one tells themself it’ll be a completely different experience. This is a form of rehearsal to rewire the brain into trusting the statement. Another option may be to continually fill the mind with distracting stimuli during the stressful time of visiting the doctor, so there is no mental space for worrying. If attention is focused on a specific thing that fills the mental capacity up, there’s no room to have other thoughts in that moment.
Big Takeaway
Fear of doctors is a major issue that needs more awareness and solutions. There is a lot of cognition involved in the process of creating and resolving this fear. This is the result of many negative interactions with a health professional. Research on the different effects that this terror has on the mind and body is called information processing, which is known as “ a search that occurs between the posing of the problem and its solution” ( Goldenstein, 2019, p. 362). Diving deeper, our research shows that fear affects different parts of cognition, lowering memory recall and negatively impacting schema processing. Schema processing is a major contributor to understanding fear in the brain. Emotions influence schemas and also lowers the accuracy of memories. Many different branches of cognition interact with each other, in one form or another, and in turn affect schema processing.
A way to change the fears is to reframe one’s schema, by altering the way they think about authoritative figures. In the Wise Intervention, the authors mentioned that removing attachment to traumatic situations helped individuals deal with negative experiences. The goal is to create new attachments with the positive by letting go of the negative. For instance, doctors help people stay healthy, so someone with a fear of health professionals should attach to the helping aspect of doctors and remove the negative feelings held towards them. By writing down experiences with the authority figures, it creates a form of self-distancing and reframes autobiographical memories, creating a new positive schema for the authority figures.
References
ames98. (2018). The location of the fusiform face area and the MT area: Damage to the fusiform face area is … Retrieved February 28, 2020, from https://biology-forums.com/index.php?action=gallery;sa=view;id=30309
Chills & Thrills: Latrophobia – The Fear of Doctors. (2018). Retrieved February 28, 2020, from https://top10md.com/chills-thrills-latrophobia-the-fear-of-doctors/
Goldstein, E. B. (2019). Cognitive Psychology: Connecting Mind, Research and Everyday Experience, 5th edition. Boston, MA. Cengage.
Walton, G. M. (2014). The new science of wise psychological interventions. Current Directions in Psychological Science, 23, 73 – 82. Doi: 10.1177/0963721413512856
Walton, G.M. & Wilson, T.D. (2018). Wise interventions: Psychological remedies for social and personal problems. Psychological Review, 125, 617 – 655. https://doi.org/10.1037/rev0000115
